


by: Tim Powell MD and John Powell MD
Evergreen Family Medicine
Post originally appeared here.
1/25/2021 Masking the Science
We have purposely avoided directly confronting the issue of masks because it is such an emotional and political issue. Like waving a red flag in front of a bull, the topic elicits strong emotions which overwhelms reason. We wear a mask in the hospital and don a N95 mask, gown and gloves when we see a patient known to have COVID-19. Masks are used for source control when patients are admitted with various types of infectious respiratory diseases. After the visit, we dispense of the gown, gloves and change into our regular surgical mask to continue patient rounds. In public, we wear a cloth mask to comply with executive orders and as a courtesy to others who feel afraid and uncomfortable. Like most of you, we rarely wash the mask, we stick it in our pockets, pick it out of the glove compartment or off the floorboard when we need it.
In truth, we wish masks worked. If they did, it would be a cheap, and easy way to control the spread of Covid. The idea that they protect not only their wearer, but also those people around them seems noble. We wished masks worked because citizens are spending billions of dollars on them.
We wish masks worked because most Americans wear them now. Telling them it was unnecessary will not make them happy. We wish masks worked because they have become a symbol for virtue and social responsibility. Anyone who doubts their utility is personally attacked; as though they don’t believe the viral pandemic is real, or don’t care about those who die from it.
We wish masks worked, because they distract from other important Covid related issues such as: school closings, lack of access for non COVID related illness, increased mental illness, elderly dying alone, missed youth experiences, substance abuse, suicides, increased poverty and homelessness, suppression of free speech, censorship of science, disruption of supply chains, government agencies used to oppress small businesses, restriction of religious gatherings, travel disruptions, isolation protocols, modeling over actual data, quarantines, lockdowns, contact tracing, and global harm of the economy that most impacts the working class, vulnerable and poor.
We wish masks worked.
But they don’t.
At least, not the cloth and surgical masks you see in the public arena. They litter the landscape and waterways. They are difficult for people with disabilities and small children. It promotes natural germaphobe tendencies and indoctrinates the young to see their fellow humankind as a sack of germs.
There have been many randomized controlled trials (RCT) and meta-analysis of previous studies that suggest that masks do not work to prevent influenza- like illnesses, or respiratory illness transmitted by droplets and aerosol particles – like Covid. This knowledge was the basis for the WHO and CDC recommending against the public wearing masks in the spring of 2020. It was repeated by authorities and experts at every level.
Dr. Jerome Adams, the Surgeon General tweeted, “Seriously people – STOP BUYING MASKS! They are NOT effective in preventing the general public from catching Coronavirus”
Dr. Anthony Fauci told 60 minutes, “There’s no reason to be walking around with a mask”.
In April, the New England Journal of Medicine wrote: “we know that wearing a mask outside of health care facilities offers little, if any protection from infection”.
What changed? Well, it wasn’t the science.
All studies are not equal. The gold standard of medical evidence comes from randomly controlled studies. Recent observational studies that were used to support mask mandates were poorly designed for confounding factors, carried out in medical environments, and then, impressions were extrapolated to the general public. Studies that evaluated the viral exposure of mice in a cage covered with mask material vs. caged mice without a mask cover does not seem to translate well to a world of humans who use their hands. In contrast, a recent Danish mask study of the general public that was performed in a prospective, randomized fashion did not endorse the current majority narrative and was vigorously criticized and suppressed by some.
A new drug, medical product or procedure would never be approved based on this type of evidence.
Logic argues against mask effectiveness. The size differential between viral particle or droplet size expelled from the human respiratory tract compared to the filter size of surgical or cloth masks is substantial. If you read the fine print on most consumer masks, one will likely read a statement such as this; “not intended for medical purposes and has not been tested to reduce the transmission of disease”.
The best studies are outcome based and measure “patient oriented evidence that matters.” A pharmaceutical company may show their statin drug greatly reduces cholesterol and science can show a correlation between cholesterol and heart disease. So, the obvious premise is that lowering cholesterol reduces risk of heart attacks.
Except it doesn’t. At least not for primary prevention in patients without preexisting vascular disease. It is why you must do the study. Does the intervention work in real world conditions?
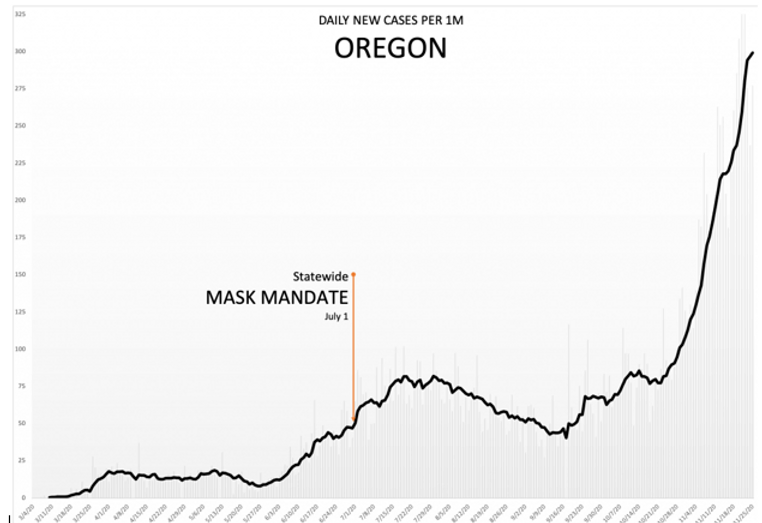
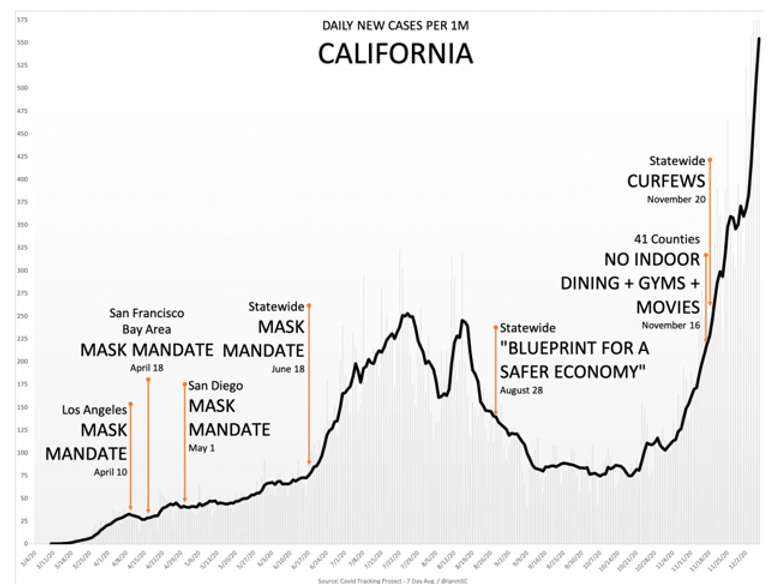
In August, Pew Research reported that 85% of Americans said they wore masks in public all or most of the time. If this is so, and if masks are effective, why has the incidence of SARS-Cov-2 increased so rapidly? Why is there not a favorable correlation between mask usage and disease transmission in countries and states with different mask policies?
If masks and lockdowns work, why don’t they work?
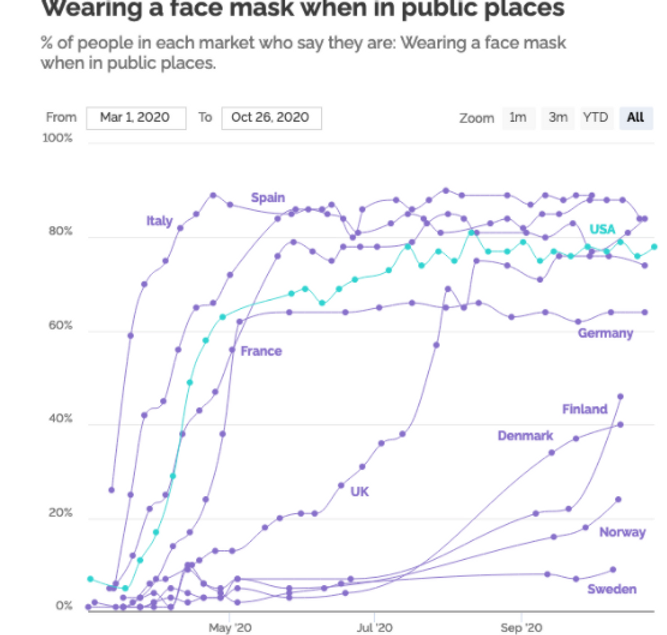
The graph below shows the daily number of deaths per million in the UK, France, Spain, Italy and Sweden from March to December. The number to the right reflects the percentage of the population that report wearing a mask in public spaces. Sweden has the lowest number of deaths per million in this comparison despite only 7.7% of the surveyed population reported wearing a mask. For those who argue that Norway, Denmark and Finland have lower mortality rates than Sweden. They would be correct, but these countries also have much lower rates of mask use compared to other European countries (less than 50%). Masks have been oversold as a solution.

Dr. Anders Tegnell, Sweden’s state epidemiologist said, “face masks are an easy solution, and I’m deeply distrustful of easy solutions to complex problems”. He was right. Sweden now (1/23/2021) has fewer deaths per million people (1086) than the United States (1284). In fact, they have a lower death rate than 30 of our states. History is replete with examples when politics or religion meddles with science and adversely impacts solutions. Dr. Martin Kulldorff has argued against widespread public mask mandates from the beginning. He is a professor at Harvard Medical School and a leader in disease surveillance methods and infectious disease outbreaks. He describes the current pandemic policy of COVID lockdowns and mask use this way; “after 300 years, the Age of Enlightenment has ended.”
At this point, many do not need an expert opinion to trust their own intuition and lying eyes that masks are not working. Everyone wants to mitigate the transmission of the virus, but let’s focus on what works.
But, wearing a mask is so easy to do. Can’t you just shut up and wear the damn mask?
Why are we poking this tiger, this mask issue now?
Because there is mass hysteria, and many are blind to it.
Because it’s an irrational and divisive policy when unity is required more than ever.
Because evidence should matter.
Because in 2019, if we saw a father struggling to muzzle a terrified, crying 2-year old child on a plane with a cloth, we would report them to authorities for possible child abuse. In 2021, we kick the whole family off the plane unless the father is successful in his efforts.
Because a young man with autism who is unable to tolerate a mask on his face is publicly shamed.
Because the masks offer a false sense of security and may adversely impact more important public health mitigation measures.
Because our local high school cross-country teams should not be running the trails wearing masks.
Because the Oregon Board of Medicine suspended the license of a physician who objected to this policy.
Because one of the greatest losses in this pandemic has been the loss of credibility of organizations for whom we held in high regard. Organizations such as the CDC, WHO and Public Health Organizations that need to maintain the trust of the citizens.
Because it is increasingly apparent that the basis for the mask mandate is not medical, but political.
Because fear and panic should not prevail over actual evidence, even when many powerful institutions have expended so much political capital promoting the wrong policy.
We wish masks worked.
We wished we didn’t have to fight about them.
But they don’t.
And we do.
Tim Powell MD
John Powell MD
If you want to see more graphs, we have included them below as well as a video demonstration.



In September 2020, the CDC acknowledged that SARS-Cov-2 could be spread in an aerosolized manner. Masks are ineffective against this mode of transmission. Early in this pandemic, some physicians showed video evidence of how masks might work as a source control for droplet transmission of COVID-19. Unfortunately, this is not the case for aerosolized transmission of viruses as demonstrated in the video link below.



[…] https://www.schillingshow.com/2021/02/02/masking-the-science/ […]